

Bottoming and IBD
Bottoming or anal sex (the fancy medical term is receptive anal intercourse/RAI) is an important part of many people’s enjoyment (not everyone’s preference, but if you like it, you like it, and IBD shouldn’t make you stop!)
Making sure your experiences bottoming are pleasurable and safe having IBD are important.
I use bottoming/anoreceptive intercourse/receptive anal intercourse (RAI)/anal/anal sex all interchangeably on this website - you may use different words, just apply whatever you use to the topic! This is because medical literature/academia/doctors use different terms (academia doesn’t use the term ‘bottom’ much, per se)
For general questions about sex, positions, and intimacy in IBD centered around LGBTQ health, see here.
More about bottoming after specific things like fissures, hemorrhoids, and more can be found on this page.
Information about PrEP, PEP, DoxyPEP and more can be found on this page.
Information about stomas/setons/other surgery can be found here. Information about bottoming with IBS and tips that also apply to IBD can be found here.
For information on coping with perianal disease and the issues it may introduce to identity, bottoming, and more, visit here.
Important: Being gay, bottoming, or any permutation of the sorts does not cause IBD (and isn’t “2 times more likely to give you IBD”). That’s not how that works and that paper was Not It.
If you love it, lube it. Proper lubrication is important for preventing excess friction and irritation and reduce the risk of pain, further soreness/irritation or hemorrhoids.
If you have IBD and identify as LGBTQ+, consider taking this survey created by physicians and patient partners in collaboration with the Crohn’s and Colitis Foundation! The survey is here
Not Very Brief Overview of Bottoming/Receptive Anal Intercourse and IBD
I do NOT want this to come off as being a party pooper (haha) or sex negative at all, far from it! I just want everyone to have the best time they can while also not compromising their IBD or gastrointestinal health! So see below, and around the website for things that you may find helpful with that.
Imodium
Prep for bottoming often involves using things like loperamide (Immodium), enemas, eating a high fiber diet which can be a big no-no in IBD (every person is different!), so be sure to double-check with a trusted care team member if taking things like Immodium and other prep such as anal douches is safe for you.You don't have to say "I'm asking about bottoming/anal sex" you can ask "Is it safe for me to take Imodium" or “I was wondering if I can take Imodium to manage diarrhea/urgency/___? (because honestly, so many people with IBD have wondered if they can)
Enemas and Douching
See more information at the bottom of the page, but in summary…
Saline (Fleet, etc) is an ideal enema to use in moderation if you do not have access to isoosmolar enemas- your body, and butt, have a very delicate balance of electrolytes that can get out of balance if you use the wrong equipment. Think about colonoscopy prep - it’s a bunch of electrolyte water!
Using Fleet enemas/douching too much can irritate your inner rectal mucosa, making it more friable or delicate- too much of anything can be a bad thing, so be careful not to do too much (everything in moderation!)Chemistry lesson!
Saline (Fleet) is HYPERtonic (hyperosmolar) and will draw the water out from your rectum/anal canal lining - similar to how some colonoscopy preps work (it’s an osmotic laxative and draws water into the colon by osmotic force.
Doing that too much, especially if you are someone who is prone to dehydration due to your IBD can be problematic, because this will promote dehydration and make you more dehydrated by pulling water out of your system.
Please don't use anything from under or above the kitchen sink like bleach, rubbing alcohol, olive oil to douche.
That would hurt your butt quite a lot - plus olive oil will make you really slippery and oily/greasy . If you need help buying lube there are places that give it away for free like sexual health clinics, and worst comes to worst, submit here and I will venmo you before you have to use bleach or some good olive oil (save that for cooking)
If you notice pain, bleeding, or unusual soreness/weeping when prepping or bottoming (engaging in anoreceptive intercourse) pause what you are doing - you may need to recollect, try a gentler approach, or have a check-in with your physician.
IBD can be associated with being on immunosuppressive medication (biologics, immunmodulators, steroids etc). so.....Protection is important if with a new partner(s) as well as being proactive about testing for STIs. See this and this page for information on DoxyPEP, STIs and IBD, and other infection related IBD sexual health things.
If you begin to notice blood or experience pain - it may be time to take a break from bottoming/anoreceptive intercourse
Akyl/Amyl nitrite/poppers act as a vasodilator and can have harmful side effects, such as methemoglobenemia, and can lower your blood pressure * a lot* and cause a rapid spike in heart rate. Be very careful when using and make sure someone is with you. Please be safe!
If you love it, lube it.
Lubricant (lube) is your friend! I cannot emphasize this enough. Spit is NOT a good lube - use water based or silicone based (unless using a silicone based toy - silcone + silicone = degrade) See this page for more info on lube, condoms and what to mix/not to mix.
Be aware of what base your lubricant is made of though - silicone, water, oil, etc. Silicone-based lubricants can damage silicone products but are safe to use with condoms. Oil-based lubricants/oil-based lube will lead to condom breakdown! This can lead to an increased risk of STIs.
PLEASE don't use anything like cooking oil, etc (Click here for more info on that)
ALWAYS use a flared base for anything going in behind - this applies for everyone, not just if you have IBD! No matter how much you think or are confident that it won't get pulled up in there, there is always a chance you are proven wrong. There are STRONG muscles in the anus!
Foreplay is important! Being turned on will help you and your butt and anal muscles relax.
Foreplay also triggers physiological and physical responses (releasing oxytocin, serotonin, etc that lower cortisol) that make the sexual activity enjoyable and possible!
This applies for everyone - not just IBD people - sex shouldn't hurt (unless you are into that, then knowing the difference between good pain and bad pain is important) and you shouldn't bleed!
If you are just coming out of a flare, you may try other positions or ways of being intimate while your bottom or rectum is healing - save those bottoms! (not to exclude tops or anything, love y'all too)
If your Crohn’s or Ulcerative Colitis is in remission, anal sex should be fine - especially using lube and being smart about safe sex. Just remember to listen to your body, stop if anything feels weird or hurts weirdly, and communicate.
You won’t have an enjoyable time if you are suffering through or in pain- but there is one piece of advice for bottoming/anal sex that is most important of all - I cannot stress enough ,
LISTEN to your body and COMMUNICATE with your partner!
Never let anyone make you feel less than as a partner because of your IBD. You deserve to be respected and cherished as you are. This disease is tough, but you are tougher.
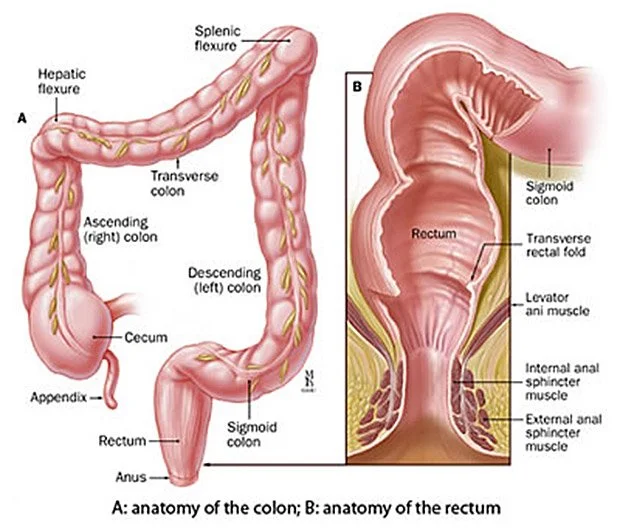
A basic diagram of colorectal anatomy that you might find in a textbook from the 80s or on your doctor’s office walls.Having a Pleasurable Bottoming Experience
With IBD
Fiber: Decreases your need to douche, BUT in IBD, fiber can be a touchy subject. It may help to ask your doctor about increasing fiber in your diet (you don’t have to say it’s for the purposes of anal sex.)
Companies market fiber supplements to bottoms - DON’T FALL FOR IT!They are soooo overpriced, and the same thing as any fiber supplement you get at the pharmacy or grocery store. Just get a psyllium husk supplement and don’t buy something that is marked up 500%.
Douching: There are no increases in STI transmission associated with douching. See here - specifically, rectal douching was not associated with increased rates of anorectal chlamydia and gonorrhoea.
Isotonic saline does not damage the epithelium. Fleet enemas are HYPERtonic/Hyperosmolar and can lead to epithelium damage after too much use and dehydration if used too much or if you are already dehydrated. Everything in moderation!
DO NOT USE those jet stream super powerful douches like shower douches. The tissue walls/lining of your rectum/anus needs more time to heal and adapt to high pressure force and that can hurt it.
See more information below about douching including how to douche, what to use, and the do’s and don’ts.
Lubricant: Silicone lubricant is ideal ONLY if not using a silicone based toy. If you think you’ve got enough lube, use some more. Iso-osmolar lubricants (typically silicone based) might be preferred for bottoming as hyperosmolar lubricants (typically water based) can cause epithelial damage and increase risk of bleeding and infection if used too frequently. Because of our IBD, we might (and usually) need to use more lube. If you love it, lube it.
HOWEVER, when using silicone lubricant with silicone objects (for example, a dildo), be careful, as combining silicone + silicone will lead to material breaking down.
Poppers: Don’t combine these with PDE5 inhibitors (medication for erectile dysfunction and pulmonary hypertension including Cialis and Viagra). Poppers should be used with a lot of caution as they can cause significant cardiac events, and if you are on certain meds to manage IBD side effects or other conditions, you may need to check that.
Here is the interaction checker for medications that interact with poppers:
Foreplay: Getting aroused/turned on will not only relax you, but make the muscles around your butt relax and blood flow increase (all the happy chemicals do that) It never hurts to throw in some foreplay to loosen things up!
You don’t need a partner for this, either - fingers are a good place to start, because you can start with a pinky and work your way up, or you can use sex toys like vibrators, dildos, anal/rectal dilators,etc https://www.drugs.com/drug-interact
Consent: Open communication, respect, and honesty all are super important to having a pleasurable experience. Consent is sexy!
Communication: Having a pleasurable time bottoming (and being a top!) should involve open communication, regardless if you have IBD. Communicating what feels good, what doesn’t, what you are comfortable with, what you aren’t, etc, is essential to having the most pleasure.
Safe Sex: Condoms and dental dams if you are with a new partner and good hygiene ALWAYS! Brush your teeth and wash your booty!
Medication: Some people are prescribed hydrocortisone cream by their PCP (there are also OTC options) for use the day before and day after to soothe and “calm down” the anus area. Some people’s IBD specialist also recommend using Uceris foam the day before and day after to handle any residual inflammation as well.
If It Hurts:
Recurrent or persistent pain that occurs before, during or after bottoming/anal
When/How Does Painful Bottoming Happen?
Painful bottoming/receptive anal intercourse of any kind) is referred to as anodyspareunia
Painful bottoming/anal sex typically occurs at the anus during initial entry or during entry and/or thrusting.
In people with IBD and dyspareunia, the missionary position can cause penetration pain during sex, so you may consider modifying positions.
Internal anal sphincter hypertonicity and sphincter spasms can result in difficulty with anal entry/penetration and painful anal sex.
Sharp pain might additionally be experienced during entry/penetration or thrusting if a penetrating object pushes on the rectosigmoid junction causing mesenteric stretching (refer to the diagram below!)
The rectosigmoid junction is roughly 6 to 9 inches (15-17 cm) up from the anus.
Some people really enjoy this area and it can feel really good! (colloquially known as the “second hole”/"second ring" etc.)
If that is your thing/you enjoy that or it feels good to you, ensuring you are maximally prepared and relaxed is a good idea.
Follow the tips above and work with your partner(s) to make sure you are ready, and don't be afraid to try things out yourself beforehand to "test the waters" - i.e, self play with a dildo at home, fingers, etc.
If you have active inflammation in this area (rectosigmoid junction/second hole) things may not feel as good and the tissue may be more prone to friability/easier to damage/bleed. If you are in a flare that is affecting this region, it may not feel as good since the area and mucosa is inflamed.
There is no research or evidence regarding sexual intimacy and effects during active IBD involving the rectosigmoid junction and how pleasure is affected in this area, but from conventional wisdom and connecting the dots, one can assume it would be less pleasurable and the tissue would be more friable/sensitive/inflamed and pain would be more likely rather than pleasure. I have no idea though!
If this is the case, take everything slow and be smart about what you do.
Trust your intuition/gut feeling (even if your guts are a little different)
Anatomical, Physiological and Psychosocial Factors That Can Contribute to Painful Bottoming
Inadequate anorectum lubrication (aka - not enough lube)
The anorectal angle (the angle of a line from the anal canal tangent to the posterior rectal wall, the angle increases after evacuation (fancy word for pooping, important in anal continence and how your sphincter functions)
More about the anorectal angle below!
There are two rings of muscles in your butt.
External muscles you can control and relax on your own, but the internal sphincter only loosens up if it senses pressure.
Tip: To help relax these muscles, you can take a finger, lube it up, loosen up your butt before you try to push anything up there.
Size of the penetrating object (whether that’s a dildo, toy, penis, finger, etc) - if it is too big (length wise or width/girth wise) you may be a bit uncomfortable. I promise your partner will understand and not be offended if you need to slow down because size is an issue.
It’s so important for not only loosening things up but dilating the blood vessels and everything down there.
Proctitis (inflammation of the rectum) may be associated with rectal pain, tenesmus and bleeding.
For us with IBD engaging in RAI/bottoming, increased bleeding from proctitis might not be life-threating, but could create anxiety for yourself (and partner(s) if present) from concern as well as confusion regarding the underlying source of the bleeding.
For individuals with prostates affected by IBD with rectal involvement, local inflammation can cause persistent prostatic inflammation (inflamed prostate area), likely affecting bottomming/RAI. This would also decrease the pleasure and enjoyment experienced by prostatic stimulation/prostate orgasms.
Psychosocial Factors That Can Make Bottoming Unpleasant
All of these things (listed below) can increase sympathetic nervous system activity that then leads to increased anal sphincter hypertonicity (AKA when you get nervous and wound up, your butthole gets too wound up and nervous too)
Generalized or conditioned anxiety (which is more prevalent in individuals with IBD, and in minority populations and LGBTQ+ individuals)
Trauma history (unfortunately, prevalent in people from sexual and gender minority communities).
Internalized homophobia.
Fear of STI transmission (including HIV).
Fear and/or phobia of engaging in a stigmatized act (related to internalized homophobia).
Defecation concerns, including defecation during RAI - these are often associated with anodyspareunia (painful bottoming/receptive intercourse)
This is all the more reason why it’s important to stay in tune with your mental wellbeing and mental health, and check in with a therapist/psychologist/psychiatrist/mental health professional of whatever flavor to make sure everything is good.IBD Systemic Inflammation and Bottoming
Widespread/systemic inflammation in IBD can also make bottoming not the best.
Systemic inflammation from IBD can cause side effects with negative impacts on things in the bedroom, including:
Bloody diarrhea
The fear of having diarrhea can also contributing to issues with intimacy, so make sure this is something you talk to your doctor about if it’s an issue important to you, and communicate to your partner as a concern (but NOTHING to be insecure or worried about - everybody poops!)
Although RAI/bottoming might initially be painful, over time, the pain generally diminishes and pleasure increases - practice and getting more comfortable with bottoming can make things go easier. This goes for everyone - IBD or not.
And most importantly, don’t let the haters (or very misinformed people) get you down! You can, in fact, bottom with IBD.
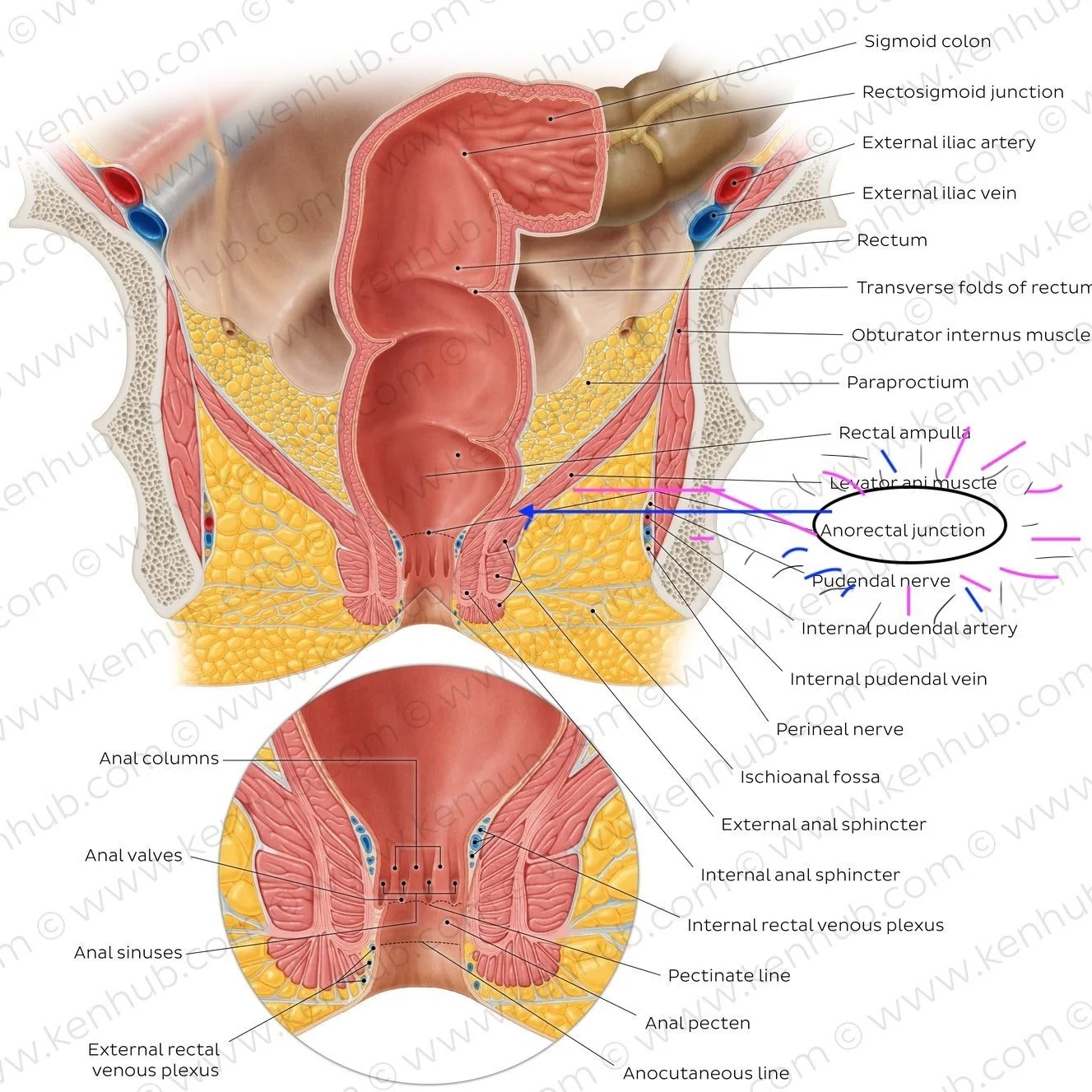
Detailed anatomy of the anus and rectum - the anorectal junction (“second hole” is circled) If your IBD is active in this area, you may not have as much pleasure here.
Basics of Bottoming: Anatomy and Physiology 101
a rudimentary overview of the A&P
What Happens Anatomically?
During anal sex, the penis (or dildo, toy, or whatever you chose) is inserted into the anus, past the external and internal sphincter muscles, and into the rectum.
The rectum is connected to the sigmoid colon, which is where poop is collected and stored by your body before you are ready to use the bathroom.
It can take 2-10 hours until it fills up after you eat and you have to defecate -meaning there’s quite a bit of time in between when you eat and when your colon fills
Although there are several factors that may affect this including IBD or IBS or if you have altered colonic transit times due to gut dysmotility conditions, etc) these are just the textbook numbers.
What is an External and Internal Anal Sphincter?
When talking about stretching the muscles for anal sex… what muscles are we talking about?
The external and internal sphincters need to stretch open, or relax, to allow entry (for a penis, a dildo, whatever the situation is).
You can control your external sphincter (skeletal muscle) consciously, while the internal sphincter (smooth muscle) is not under voluntary control.
As a result, the internal sphincter may need some additional coaxing to relax.
Think about it - when you have to poop sometimes it just comes automatically, and sometimes you have to push it out!
This is one difference between smooth muscle versus a skeletal muscle (there are a lot more, but let’s not rehash A&P)
When people experience pain during anal sex, a simplified reason may be that the external sphincter is not relaxed before their partner’s penis goes in (or dildo, or toy, etc).
Nerve Endings
Nerve endings produce sensations through even light touch or pressure by transmitting information from an external stimulus to your brain - we have these all over our body, from our skin to our colon and rectum.
In the anus, there are nerve endings that produce pleasure (or pain) - which is what we are aiming to avoid!
Foreplay can help you begin enjoying the sensations around your anus, and also help to relax your sphincter.
If you are having trouble relaxing around there, you can try exercises to help.
When you’re alone, or with a partner if comfortable doing so, use light touch around your anus to help relax, different types of touch, different types of pressure, and explore what feels good.
Keep going for as long as you enjoy it.
Some people can be overly sensitive around their anus, and can benefit from desensitization exercises.
To help desensitize, apply deep, broad pressure, such as a flat hand, around your anus to help calm your nerve endings down first.
Lighten up the touch and see if you can ease your mind and learn to enjoy the touch around your anus.
If you are recovering from a flare or perianal disease, you may be more sensitive in this area, so things may take more time! And that’s okay.
Pelvic Floor
People with IBD and GI disease may already be familiar with the term pelvic floor (muscles that support the pelvis) or be referred to pelvic floor PT, due to how the disease can impact our pelvic floor muscles and continence and the like.
Everyone has a pelvic floor, and it is intricately linked with how you pee, how you poop, your “core stability,” and erectile function (for people with a penis).
Will most people feel the muscles in the pelvic floor? Probably not.
But just as you feel the motion of your knee extending (this sense of your body moving (proprioception) and can identify your quadriceps performing that motion, you can become aware of the muscles of the pelvic floor.
The pelvic floor has two states of motion: it can be in a contracted state of motion (a Kegel) or relaxed state of motion.
These are also associated with different states of mind: very relaxed, normal day-to-day, and high stress or anxiety.
See here for more information on pelvic floor physical therapy.
When preparing for anal sex and bottoming, it’s best to be relaxed, and to also begin to play with constriction, relaxation and bearing down with the pelvic floor muscles.
The Unique Shape of Your Rectum!
Your rectum isn’t a straight tube, there’s a bend in your rectum called the “anorectal angle.”
Imagine a long balloon that is twisted at a 90-degree angle about 10 centimeters from the end of it.
This is the shape of your rectum, that allows poop to be held back until you’re ready to go to the bathroom.
(This is also a rudimentary definition of anorectal angle)
During anal sex, it’s best if the anorectal angle relaxes slightly so that the rectum becomes more linear.
You can make this happen/relax it more by using your pelvic floor muscles to “bear down” during sex (hear me out - there is a scientific reason)
Bearing down or pushing out, like the feeling when you’re pooping, as the person topping is inserting whatever object (penis, dildo, etc). (aka, push out as the person topping pushes in) helps straighten out the anorectal angle
This works by bearing down through your pelvis without tightening your external sphincter (this is where the pelvic floor muscle control comes into play)
This will allow your anorectal angle to be more linear because your pelvic floor muscles will be relaxed.
This allows the muscles to elongate and adapt to changing sizes.
The person topping will feel less resistance/ it will be easier for them upon entry.
Your rectum: Is there poop in it?
Generally, No! Unless you have special circumstances (like, you have diarrhea or steatorrhea (excess fat in your stool, could be caused by things like medications, malabsorption, bile acid malabsorption, exocrine pancreatic insufficiency, or simply just eating a high fat meal.
People generally assume is that there is feces (poop) just inside their internal sphincter/ in their rectum (their butt). This is a fair assumption!
As with everything, some exceptions do apply, but for the most part, poop does not stay in your rectum.
Poop is stored in your colon until you’re ready to use the bathroom.
Right before you have to poop, there will be poop/feces there, but otherwise, there isn’t just poop lurking in your rectum.
Unless you are reaaaaally constipated (then please let your doctor know, and you would have to be really, really constipated)
When you’re sitting on a toilet, poop travels from your colon through the rectum and out your anus.
Some people still prefer to douche their rectum before anal sex (more on this below), but you should know that even if you don’t douche there may not be any poop (depending on the consistency) in your rectum.
There may be some fecal matter residue if you recently pooped and didn’t wipe very well (or use a bidet, seriously, try them out!) but you really don’t have to worry about poop in your rectum.
Be comfortable with the idea that sometimes poop comes out of your butt.
If you have IBD, there is a good chance you have come to terms with that, but it can be embarrassing regardless.
If you’re afraid of that idea, you can stick with oral sex or you can work on getting comfortable with the idea that it might happen.
If you’re overly worried about poop showing up during sex, you’re going to shock your system into an anxiety-ridden state that can negatively affect the sex you’re having and you won’t have a good time.
Keep in mind that caffeine and foods high in fiber can accelerate mobility to the lower bowels, though.
Leave some time before sex (maybe an hour or so) if you’re going to douche.
Mindset
In everyone, IBD or IBS, or no IBD or IBS, digestive disease or not, anal control consists of both voluntary and involuntary muscles.
It’s used as an analogy in things like sports (and debate team and apparently LinkedIn…), but I think it works here too - mindset is 80% of the challenge. The other 20% is skill, strategy, and what you know and can do. Your mindset influences your response emotionally and psychologically and if you are in a bad mindset, you will probably have a bad time.
If you’re afraid, anxious, worried or fearful, your sympathetic (fight or flight) nervous system takes over, which can result in a very negative experience your body will remember.
Unfortunately, people with IBD and minority populations tend to report higher levels of anxiety and worry, which probably leads to more of this “fight or flight” system in action.
The mind body connection is vital in creating positive experiences, so being aware of what state your mind is in will express how your body reacts!
It’s best if you are fully relaxed, and that includes your anus!
Taking deep breaths can help, but mostly, trust with your partner is paramount.
This is why it’s important to take time to relax, prepare yourself, and get into the right frame of mind so that you’ll enjoy the sex you have and ensure you have healthy communication with your partner(s) and trust them.
Benefits of Intimacy/Bottoming (other than the obvious)
Benefits of Intimacy/Bottoming (other than the obvious)
Sex is good for you!
Sexual activity is a fundamental human function with short-term and long-term emotional, social, and physical benefits. (but it’s also important to keep in mind that while good sex promotes good health, good health also favors good sex.)
Short Term Benefits
Many of these occur immediately following sex.
One example is the increased pain threshold after direct genital stimulation
Associated phenomena with intimacy, such as affectionate touch is also known to have powerful beneficial effects on its own, such as cardiovascular relaxation
Interpersonal touch not only promotes well-being and emotion-regulation but also facilitates neurocognitive processes underlying flexible goal-directed behavior (i.e., cognitive control)
Positive sexual experiences has a lot of overlapping beneficial outcomes!
This includes pleasure, pain reduction, sleep improvement, and improved function of the immune system (the last one with also intermediate-term benefits).
Pleasure, pain reduction, and increased mental health quality of life is attributed to the production of three of the major intervening hormones: oxytocin, testosterone, and cortisol.
Pleasure (Happy Chemicals)
The most obvious and distinctive short-term benefit of sexual activity is sexual pleasure.
This may include solo or partnered behavior as well as cognitive experiences of sex, such as fantasies.
Non-penetrative sexual acts, such as oral and manual stimulation are quite common, especially among sexually diverse and gender-diverse individuals and may be more pleasurable than penetrative sexual activities.
While it is subjectively rewarding, it has been linked to overall well-being
Sexual pleasure and its associated positive emotions functioned to reinforce sexual behavior and to enhance self-esteem, resulting in a beneficial cycle.
Pain Relief
Sexual activity can be used as a strategy for reducing pain as well.
In migraine patients, 60% reported an improvement of their migraine during sexual activity (within 70% of them moderate to complete relief).
Sexual intimacy might alleviate pain by providing a source of distraction as well as other pathways.
One study found that pressure stimulation of the anterior vaginal wall and self-stimulation of the clitoris had an analgesic effect, reaching maximum effect with orgasm.
Endorphins and oxytocin might also explain the pain-reducing effect of sexual activity.
Higher oxytocin levels are correlated with a higher pain threshold , with muscle relaxation contributing to the pain-reducing effects of sexual activity.
In patients with multiple sclerosis and spinal cord injury, sexual vibration and orgasm can produce reductions in spasm and muscle relaxation that last for several hours.
Sleep Improvement
Sex may promote health through sleep-related pathways!
Studies have found links between good sex and good sleep, but the causal direction is unclear. (correlation doesn’t always directly equal causation, etc. etc.)
Empirical evidence (and conventional wisdom) suggests that sexual activity followed by orgasm facilitates sleep, although laboratory studies have not verified this causal hypothesis
Masturbation also seems to help assist in inducing sleep.
In an Australian study among >750 individuals, more than 50% indicated improved sleep quality after masturbation to orgasm, with no gender difference.
After sex with a partner, the sleep benefits were higher.
Allergies/Immune System
Studies focusing specifically on other forms of sexual activity have found that masturbation was followed by a transient increase in the absolute number of leucocytes, in particular killer cells, that can be seen as a “boost” of the immune system.
Kissing, which remains a nearly ubiquitous part of sexual expression, appears to alleviate allergic symptoms by decreasing allergen-specific IgE production.
This does not mean you should stop taking Claritin and substitute that for a kiss. Integrative medicine is the new thing - complimenting your traditional treatments with others :)
Intermediate Term Benefits
Ejaculate contains many substances that are easily absorbed by the epithelium, especially in highly aroused individuals and associated with decreases in depression and anxiety (testosterone,DHEA, and zinc
The free testosterone level (i.e., testosterone’s bioavailable fraction) in seminal plasma is 3 - 4× higher than in the blood , potentially increasing the antidepressant properties of the hormone
Engaging in sex appeared to create mood-driven positive outcomes the following day as well.
One study found that physical affection or sexual behavior in couples significantly predicted next-day reductions in negative mood and stress, and next-day increases in a positive mood.
Long Term Benefits
Masturbation actually more effective than Kegels in strengthening the pelvic floor! (Penis-root masturbation)
Masturbation is positive outcomes in pelvic floor health for people assigned female at birth as well as male at birth - decreasing urinary incontinence issues and fecal incontinence issues and strengthening the muscles in the pelvis
Physical Exercise
The more physically active forms of solo or joint sexuality can indeed be seen as exercise and accordingly have the potency to positively influence cardiovascular and cerebrovascular health.
The typical energy expenditure during penetrative intercourse is ∼85 cal or 3.6 cal/min when at a moderate intensity
Even without muscular activity, sexual arousal activates circulation and can be accompanied by changes in heart rate, blood pressure, and peripheral vascular responses.
Orgasm is always accompanied by a rise in heart rate (20–80 beats/min), systolic blood pressure (25–120 mmHg), and diastolic pressure (25–50 mmHg)
As physical activity is recognized as an important lifestyle factor delaying the development of atherosclerosis and cognitive decline, and sexual activity through both arousal and intercourse achieves this.
it may be appropriate and beneficial to include regular sexual activity in health recommendations, since it is hitting all of the benchmarks of exercise (rise in heart rate, circulation, etc)
Longevity
A large, longitudinal US study found that sexual activity, quality of sexual life, and interest in sex were positively associated with health in middle age and later life
The English Longitudinal Study of Aging also explored associations between sexual activity and cognition in adults aged 50–89, finding that regular sexual activity was linked to slower cognitive decline, memory and executive function.
It’s not exactly clear from these studies whether intercourse is singularly beneficial, or whether it is the overall experience of arousal and orgasm that is beneficial (in which case solo masturbation could convey the same effects)
More research is needed to clarify a causal relationship direction though (correlation doesn’t necessarily mean causation :)
Protective Factors Against Disease
With respect to prostate cancer, studies have found that frequent ejaculation is associated with reduced prostate cancer risk and plays a beneficial role in the etiology of prostate cancer.
Regular ejaculation appears a preventive factor in the development of chronic non-bacterial prostatitis.
The overall impression is that an increasing amount of elements of sexual action and intimacy and interaction appears to favor physical and mental health - good sexual health favors good physical health, and vice versa!
So in the words of Marvin Gaye (with protection when needed and following guidelines from your healthcare team) … get it on! It’s good for you!
This DOES NOT mean to stop taking your medicine and substitute Entyvio (or Stelara, or any of the other IBD meds) or Zyrtec for any of the above.
Sometimes a little integrative medicine is key and makes the difference - combining different healing practices is a fairly effective strategy!
Douching
How to douche: summarized
What is douching?
Anal douching is the process of cleaning out your anus before penetrative play, but there’s not exactly a step by step guide for it!
Douching is the practice of squirting a water solution into a part of your body for cleaning (and “douche” can also refer to the specific device for douching, or a person who is not very nice)
Douches (often referred to as enemas or anal enemas too) are a common practice for the receptive partner before anal sex, to clear out the anus of fecal matter when preparing for anal intercourse.
Sometimes individuals with vulvas use douches to clean out the vaginal opening or get rid of vaginal odor; however, this practice can actually upset the balance of healthy bacteria (vaginal flora) and increases the risk of yeast infection, bacterial vaginosis, and pelvic inflammatory disease (PID).
Most gynecology experts and health-care organizations do not recommend vaginal douching as a part of feminine hygiene due to this. Cleaning with water and a gentle soap is enough.
Why do some people consider douching?
Anal douches allow you to clear fecal matter out of your anus, and many people who are sexually active use douching prior to anal penetration (but it may not be all that necessary!)
Anal douches are NOT necessary before anal play!
Your rectum muscle retains most of your fecal waste deeper within your intestinal tract until it’s time for a bowel movement, which helps keep anal sex relatively unmessy (of poop).
In addition, douching isn’t necessary for strong sexual health.
A small amount of waste is perfectly normal during anal sex and isn’t dangerous as long as you clean up afterward - everybody poops (not that you should be pooping during sex necessarily) but nobody has a 100% sterile body, free of evidence of bodily functions. That would be weird.
Things to consider before douching
Anal irritation or tears: Use lube and a gentle touch when inserting tools into your anus for douching, otherwise you can irritate or tear the delicate skin of your anal opening ; this is particularly important for people with IBD who are recently recovering from rectal or perianal disease and have sensitive tissue in the rectal area.
This irritation can cause pain (especially during sex or penetration with sex toys) and can put you at a higher risk of bacterial or sexually transmitted infections (STIs) and other health problems.
Lining damage: The lining of your anal canal is much more sensitive than your skin, so a harsh tool, too strong a jet of water, or water that is too warm or too cold can cause irritation, lining damage, burns, or cramping. This is one of the reasons why (as listed below) I am not a big fan of the shower hose douche.
Electrolyte imbalance: Your rectal and anal canals are filled with healthy bacteria and a specific balance of electrolytes to help regulate your digestive health; if you douche too strongly or too often, you can upset the ecosystem in your anal canal and put yourself at a higher risk of infection.
Plus, with IBD, we may be more prone to getting dehydrated (I know I am), so you don’t want to overdo it.
Step by Step Guide
Choose your method. There are several safe methods for anal douching. The most common types of douches are bulb douches (small squeezable spheres that you can fill with solution - PREFERABLE) and shower douches (or special attachments that you can connect to your shower).
Other options include drug-store enema kits, water-bag douches, and mucous suckers.
Avoid store-bought douching kits that include laxatives, since these can cause cramping or stomach problems. (No senna, ducolax, etc - see below)
Prepare your tool. Make sure to clean your device properly before use.
Rinse the components in clean, cool water to make sure you’re not introducing any bad bacteria into your anus.
Most people who douche use lukewarm, chemical- and soap-free water to douche. Your butt cannot take hot water or cold water - it is very sensitive tissue!
If you know your digestive system is especially sensitive to imbalances, consider making a homemade saline solution out of one-half teaspoon salt and one cup of water to mimic the electrolyte balance in your body. ( nice guide on how to make saline solution here)
Sit over the toilet or tub. Since water will come out of your anus during the douching process, get in position over a toilet or bathtub to catch and properly dispose of the spill.
Apply lube to your anus. If you’re using an enema bulb, which has a nozzle that goes into your anus, apply lubrication to your anus and the tool to avoid any discomfort or tearing.
You may want to apply lube to your finger and insert it into your anus to loosen your sphincter for the nozzle.
Gently insert the water. Introduce a gentle stream of lukewarm water into your anus.
Never use hot water or very cold water, since these can cause burns or cramping!!
The process for inserting water will depend on the tool you use. I don’t recommend using the shower one for reasons discussed below, but you are an autonomous adult who can make your own decisions, so just be careful!
If you have a bulb douche, insert the nozzle into your anus and squeeze gently to insert the water; once your anus feels full or the bulb is empty, keep pressure on it with your fingers and gently remove it (if you release the pressure before you remove the bulb, it will suck some of the water back into the bulb). If you’re using a shower douche, start the jet on the lowest water pressure setting and ensure the temperature is lukewarm or cool, then align your anus with the jet to insert the water. Keep the water going until your anus feels full.
Allow water to spill out of your anus. Over the toilet or bathtub, allow the water to gently squirt from your anus until your anus feels empty. The water should look dirty or cloudy and have waste in it.
Repeat until water is clear. Repeat the water-insertion process two to three times or until the water that comes out of your anus is clear.
Clean around your anus. Use a piece of toilet paper or a quick shower to rinse around your anus and clean up any remaining waste. If you choose to use soap, make sure it’s a mild soap that won’t cause irritation, and keep it external rather than internal.
Wait. While you can engage in anal intercourse immediately after douching, most people who douche recommend waiting at least thirty minutes to allow any excess water to leave your anus.
Give your anus time in between douches. Since douching can be harsh on your body and upset the delicate balance of your digestive tract, limit douching to two to three times per week. Over-douching can put you at a much higher risk for health problems.
Remember that it’s impossible to be completely poop-free. Poop and poo particles are a normal part of your digestive tract, and it’s common for some fecal matter to be present during anal intercourse, even after douching. Don’t sweat it if there is a little bit hanging around, that’s where it tends to be!
To summarize the DOs and DON’TS and MAYBE’S and I DON’T REALLY KNOW’S about douching and IBD…..
DO’s:
Using the right type of liquid to clean out your butt is important. Your body maintains a delicate balance of electrolytes to function normally - you are definitely familiar with this if you have had to get IV hydration after being dehydrated from puking/diarrhea from IBD.
If you use the wrong liquid, you can cause imbalances that harm your body - just like when you get too dehydrated from pooping or vomiting.
Tap water is fine if you aren’t using it every day, but if you do use it too much you can cause an electrolyte imbalance that using normal saline would prevent. I do totally understand not having access to the “ideal” things, so use your best judgement.
DO: Use Normal Saline. Normal saline is one of the safest solutions that can be used to stimulate defecation. There is no risk of water toxicity because it has the same osmotic pressure as the intestinal fluid.
DO: Be mindful before you douche. If you are just coming off of a flare, have underlying colitis or perianal disease, active rectal or anal infections, or active HPV, douching may irritate your symptoms or disease further. In this situation, douching may further irritate the rectum/rectal and anal tissue if you use something too abrasive.
DO: Double check what your enema solution is! Common enema solutions may contain either biscodyl or sodium phosphate, which are both rectal stimulants - it’s important to read the back of the box and check what you are buying. There are so many different kinds of Fleet enemas (they are really branching out) so it’s important to make sure you know what you are getting (the OG Fleet enema is Saline/ Dibasic + Monobasic Sodium Phosphate Monohydrate)
DO: Look for normal saline with pre-lubricated nozzle! If getting a Fleet enema (they have a billion versions), get the one that just has normal saline with pre-lubricated nozzle tips, which is less likely to cause tearing or other damage. The volume is also smaller so you are less likely to overdo it.
DO: Check the temperature! The mucosal lining of your intestines and colon is much more sensitive to temperature than the skin on the outside of your body. You may be able to tolerate a hot shower, but you’ll burn your insides if you use that same temperature in an enema. Test the water temperature first with your hand and turn down the temperature until it feels lukewarm. Then turn the temperature down just a bit more. That’s what can go up your butt.
DO: Use lukewarm water. This is preferable over cold or hot water. Cold water, while safe, is not terribly pleasant and is uncomfortable, and hot water can potentially burn if hot enough.
DO: Learn your angles and positioning when douching! Bending at the waist (this straightens the rectum, making it easier to get liquid where it needs to go.
DO: Add some lube. Place lube on the tip of the device to prevent local trauma to the area (if you don’t have a pre-lubricated nozzle).
DO: Insert the tip, but not too far of whatever you are using to douche into the rectum(otherwise water goes too far in and you pull down unformed stool into the very area you want to cleanse)
DO: Use bulking agents instead of laxatives (if your healthcare team says that’s okay). Other bulking agents like fiber supplements are better and okay. They might help you normalize your stool if you’re constipated or help you get all of your poop out at once. If you have loose stools or diarrhea, fiber supplements can help. Again, everyone with IBD has a different journey and situation.
DO: Be kind to yourself and don’t beat yourself up mentally if there’s a little accident. It’s anal sex, and you are kinda near where poop hangs out so there is always a chance a little poo makes a surprise appearance sometimes, and you shouldn’t feel dirty or ashamed. Sometimes sh*t happens, as they say.
DONT’s
DON’T: Overuse enemas. Never more than once a day, and 2-3 times a week is probably a good maximum. This is because overusing enemas can cause the OPPOSITE effect of what we want (paradoxical effect), leading to chronic constipation and losing the muscle memory in your muscles that help you poop. Douching too frequently and using products with excessive additives in areas of pre-existing inflammation can lead to bleeding and irritation. Saline douches can be irritating as well.
DON’T: Douche after sex! The urban legend that “Douching after sex will help me avoid sexually transmitted infections” is just that - an urban legend. Douching after sex does not decrease the risk of getting a sexually transmitted ifnection and has no proven health benefit. The opposite is actually true!
DON’T: Use shower enemas. (using the shower hose) It can be convenient, but due to variations in water pressure and temperature, you may run the risk of burning yourself or hurting yourself if it comes out too much/too hot/too fast. I will also add , as someone who took classes in water microbiology with PI that studied water pathogenic microbiology including what we use to shower - I really, really would not.
The high water pressure can be very hard on the tissue/lining of the rectum and anus, and it is easily damaged especially if you are fresh in remission (the high force exerted by jet stream shower douches exerts force on the tissues and area. The tissue in the rectum and anus needs TIME to adapt to stronger pressure and stimuli. *If you reaaaally want to though, just don’t put the nozzle or head of the shower head thing into your anus please.
DON’T: Use lidocaine gel or cream on your butt exclusively to bottom/foranal sex. This will numb the area and you won’t be able to feel pain, and won’t be able to feel if something is going wrong/you’re getting hurt.
DON’T: Use anything from below or above the kitchen sink. This includes olive oil, bleach, butter, alcohol, or anything else that you find under your kitchen sink. These will cause significant harm to your butt. If you are having trouble affording stuff, there are sexual health clinics that can help you find resources, and worst comes to worst, contact me and I will help. You are great, I am sure of it, but you are not the Martha Stewart of Fleet and Normal Saline.
DON’T: Frequently use tap water/soap suds if you have the option not to. Tap water is a hypotonic solution and should not be repeatedly used due to the possible development of water toxicity or circulatory overload. Tap water can be used to stimulate defecation. Soapsuds (castile soap) can be added to tap water to stimulate peristalsis.
DON’T: Use laxatives as a way to prepare for anal/bottoming. (unless you’re constipated and your doctor says to use them):Laxatives irritate the lining of your intestines, and they’ll give you abdominal cramping which can end up ruining sex. Also, they might just end up forcing more poop out that wouldn’t have come out otherwise.
DON’T: Overuse Hypertonic solutions to douche (the hypertonic Sodium Phosphate Fleet Enema). The hypertonic solution draws water into the intestines, which promotes defecation. Fleet enemas are the most commonly used and most easily accessible (the OTC brand/Walgreens/CVS brand is just a green box that is the same ingredients)
The solution is hypertonic and thus, draws fluid into the bowel, softening and loosening the fecal mass.
Hypertonic solutions are NOT GOOD for a dehydrated individuals so if that is you, or your IBD makes you dehydrated or prone to it, be aware of this.
It will make the dehydration worse due to the intestines pulling water out of the system.
DON’T: Use Fleet (a sodium phosphate enema) if you have a KIDNEY DISEASE (like chronic kidney disease/CKD)! This is because of the way Fleet works - it can disturb your electrolyte levels in a very unsafe way because of how they pull electrolytes out, leading to eGFR decline, AKI, and nephrotoxicity.
DON’T: Use Fleet (sodium phosphate kind) if you have a HEART DISEASE! Fleet is an alkalinizing agent and can cause sodium and water retention and result in hypernatremia, hypokalemia, hyperosmolality, edema and aggravation of congestive heart failure. Sodium- containing alkalinizing agents (classic Fleet) ( should not be used in people with hypernatremia or fluid retention.
The Classic Fleet saline enema
HYPERtonic
Ingredients:
Monobasic Sodium Phosphate Monohydrate
Dibasic Sodium Phosphate Heptahydrate
Do not use
For more than 3 days in a row (you’ll poop too much and get dehydrated)
You are on sodium-restrict diet
If you have heart problems (Fleet is an alkalinizing agent containing sodium and can induce sodium and water retention and result in hypernatremia, hypokalemia, hyperosmolality, edema and aggravation of congestive heart failure)
When abdominal pain, nausea, or vomiting are present. If you are vomiting, this will make you more dehydrated.
With IBD, the abdominal pain factor may be hard to discern because some people have abdominal/visceral hypersensitivity and it always kind of hurts, but if it hurts in a weird way or abnormally or something doesn’t feel right, trust your gut and don’t go any further.
If you notice symptoms of dehydration, stop using it. Symptoms of dehydration include feeling thirsty, dizziness, vomiting, urinating less often than normal.
If no bowel movement or no liquid comes out of the rectum after 30 minutes, call your doctor because you can get dehydrated very quickly.
Fleet Enema Extra®
HYPERtonic
Same ingredients (chemically) as the classic but Fleet Enema EXTRA® has 70% more volume than the standard Fleet Enema.
Monobasic Sodium Phosphate Monohydrate, 19 g
Dibasic Sodium Phosphate Heptahydrate, 7 g
Because it is just a Supersize Me™ version of the original Fleet, the same precautions and warnings apply as above.
This one will dehydrate you faster and easier because of the higher salt content, so be very careful if you aren’t very hydrated.
Fleet® Mineral Oil Enema
118 mL of 100% Mineral Oil
Do not use when abdominal pain, nausea, or vomiting are present (unless directed to by your doctor or healthcare team)
Generally just don’t use this one.
Should produce a bowel movement in 2-15 minutes (mineral oil works faaast)
DO NOT USE IF:
You have abdominal pain, nausea or vomiting
A sudden change in bowel habits lasting more than 2 weeks
Already used a laxative for more than 1 week
You have a hypersensitivity reaction.
You have a colostomy, ileostomy, appendicitis, ulcerative colitis, or diverticulitis. Mineral oil may lead to seepage and reduce the body’s ability to absorb some nutrients for people with UC.
Currently taking a stool softener laxative
if constipation continues after one week of use, contact your doctor.
Stop using it and contact your doctor or healthcare provider/team if:
You notice rectal bleeding after using this enema
You have no bowel movement within 15 minutes of using it
Don’t use this one to douche in general.
Fleet® Bisacodyl Enema
Stimulant laxative
Works in 5-20 minutes
Sodium phosphate-free and latex-free.
Bisacody, 10 mg
Also generally don’t use this one (unless you’re like, actually constipated maybe? but still ask your doctor)
Do not use when having abdominal pain, nausea, or vomiting are present (unless directed to by your doctor or healthcare team)
STOP using it and let your doctor know if you have:
Rectal bleeding.
No bowel movement within 20 minutes of using it.
Using laxatives (like bisacodyl) is NOT a great idea.
Stimulant laxatives, like bisacodyl induce intestinal contractions to help move stool through your bowel.
Laxatives can cause some not-so-sexy side effects, such as gas, cramping, and diarrhea, which can also lead to dehydration (the issue that we can sometimes deal with a lot in IBD, and one of the barriers to douching in IBD.)
Don’t use this one to douche in general.


